Massive forced civilian displacements, violence, and unmet medical needs in the Democratic Republic of Congo, Somalia, Iraq, Sudan, and Pakistan, along with neglected medical emergencies in Myanmar and Zimbabwe, are some of the worst humanitarian and medical emergencies in the world, the international medical humanitarian organization Médecins Sans Frontières (Doctors Without Borders – DWB*) reports in its 2008 list of the “Top Ten” humanitarian crises. The report underscores major difficulties in bringing assistance to people affected by conflict. The lack of global attention to the growing prevalence of HIV-tuberculosis co-infection and the critical need for increased global efforts to prevent and treat childhood malnutrition – the underlying cause of death for up to five million children per year – are also included in the list.
DWB began producing the “Top Ten” list in 1998, when a devastating famine in southern Sudan went largely unreported in U.S. media. Drawing on DWB’s emergency medical work, the list seeks to generate greater awareness of the magnitude and severity of crises that may or may not be reflected in media accounts.
SOMALIA: HUMANITARIAN CATASTROPHE
Already struggling to survive with little or no access to even basic health-care services, Somalis experienced some of the worst violence in over a decade in 2008, with people in the central and southern parts of the country living under increasingly deteriorating humanitarian conditions. While difficult to verify, given the collapsed health-care system, Somalia has some of the worst health indicators in the world: one in ten women die during childbirth and more than one in five children die before their fifth birthday. The impact of the war on childhood malnutrition was exacerbated by skyrocketing food prices and a prolonged drought in the country.
Since fighting between transitional federal government forces, supported by the internationally backed Ethiopian troops, and an array of insurgent groups began in December 2006, the United Nations estimates about one million Somalis have fled their homes. Intensifying combat in one of the capital’s most populated residential areas resulted in a surge of wounded civilians and once again displaced thousands of people. In Mogadishu, DWB treated nearly 2,300 patients for injuries caused by mortar rounds and bullets from January to late November, underscoring the fact that hundreds of thousands of civilians live in a war zone. To the north in Galcayo, a relatively calm city in comparison to the capital, a DWB team still operated on or treated more than 500 victims of violence in 2008.
On the road from Mogadishu to Afgooye, where many have been forced to flee from violence, there are more than 250,000 displaced people living in appalling conditions. Since January, more than 9,500 children were treated for malnutrition by DWB medical teams. The population is largely dependent on external food aid, but assistance is provided intermittently, and families fleeing violence are met with a lack of shelter, food, and health care.
Somalis are taking extreme risks to leave the country, mainly heading south into Kenya. There are currently 200,000 refugees, according to the UN High Commissioner for Refugees, in three camps in Kenya. Recently, an additional 35,000 arrived at these camps. Those who are unable to seek refuge in Kenya make their way north, where many have risked their lives boarding smugglers’ boats to cross the Gulf of Aden to reach Yemen. According to UN figures, more than 43,500 people – mostly Somalis, but also Ethiopians fleeing hunger and persecution – attempted the journey in 2008. Passengers say that more than 100 people are routinely packed into the 30- to 40-person vessels. Many suffocate while others drown before they can reach the shore. Since the beginning of 2008, DWB teams in southern Yemen have treated more than 8,000 people who have arrived by boat.
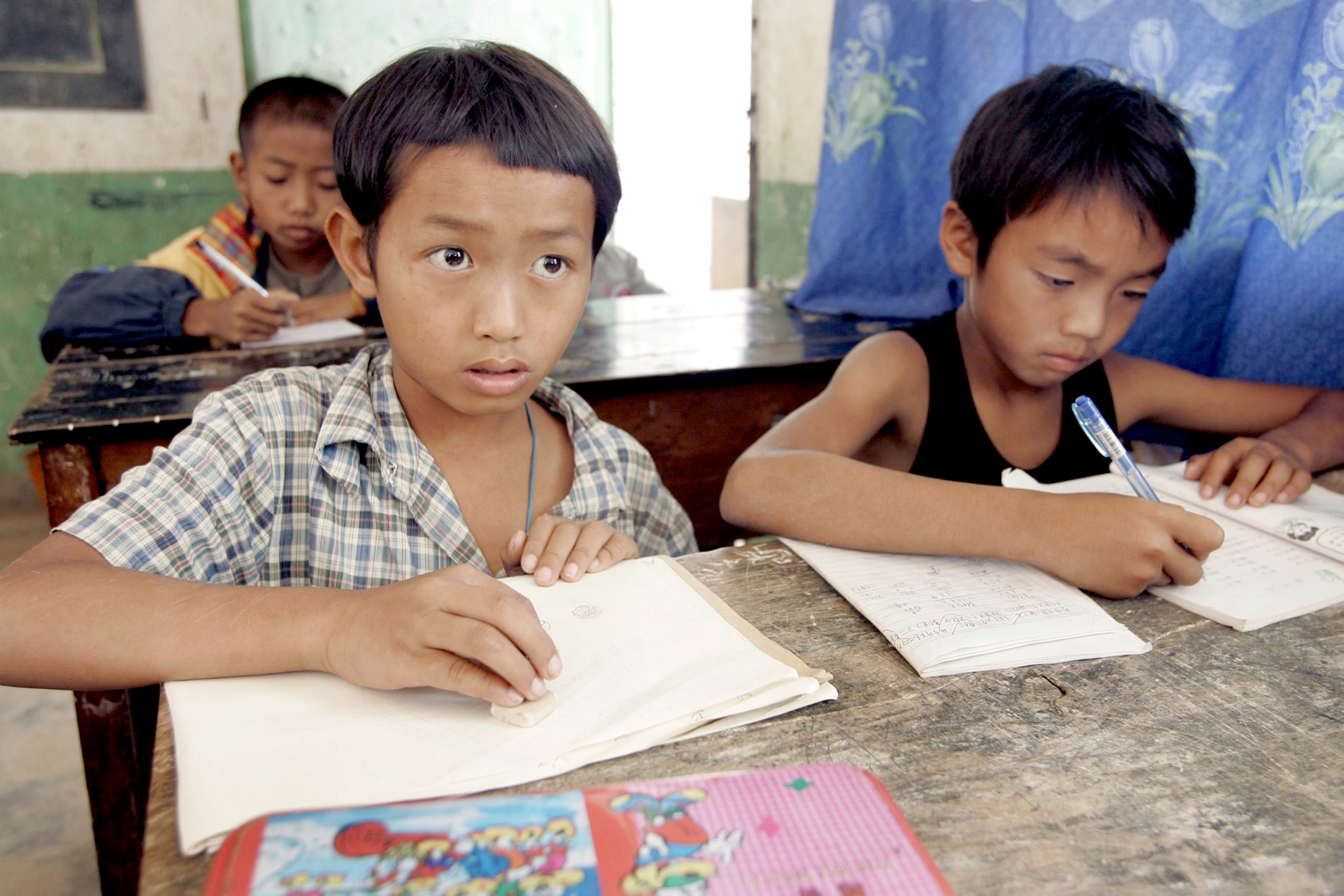
MYANMAR: A FORGOTTEN PEOPLE
On May 2, 2008, Cyclone Nargis, in all its horror, threw Myanmar back into the international spotlight, devastating the Irrawaddy Delta and leaving an estimated 130,000 people missing or dead. Governed by a military regime since 1962 and enduring low-intensity conflict in certain areas, the disaster was the latest blow to a people largely forgotten by the outside world. Meanwhile, chronic and urgent health needs remain unmet throughout the country, compounded by a lack of investment by both the government and the international community. State health expenditure was $0.70 USD per person in 2007, just 0.3 percent of the country’s gross domestic product. The level of international humanitarian aid was around $3 USD per person, the lowest rate worldwide. The selective blindness to countrywide needs, not least in the areas of HIV/AIDS, tuberculosis, and malaria, continues to cost the lives of thousands of people year after year and demands attention.
Nargis prompted an international outpouring of aid, as news of the extent of the disaster trickled out of the country. Within 48 hours of the cyclone hitting, DWB teams began providing emergency assistance to people in the worst-affected parts of the largest city in Myanmar, Yangon, and the Delta. Since then, around 750 rotating staff has assisted more than half a million people in responding to their emergency needs; providing food, shelter, water, health care, psychosocial support, and relief supplies. The majority of this aid was delivered, thanks to the tireless efforts of DWB’s national staff, as the regime refused to grant visas for additional expatriate emergency staff for several weeks after the disaster. As the situation stabilized and the number of NGOs present in the Delta significantly increased, DWB was able to hand over many programs. However, adequate assistance remains limited in some harder to reach areas, particularly in the southern parts of Bogaley Township, where DWB continues to work. DWB continues to monitor the nutritional situation in the Delta. Sadly, the struggle to get an appropriate level of assistance for Myanmar’s most vulnerable people is one that extends throughout the country.
In distinct contrast to the efforts made on behalf of the victims of Cyclone Nargis, the government of Myanmar and the international community have all but ignored HIV/AIDS treatment, a disease that claimed 25,000 lives in 2007 alone. An estimated 75,000 people urgently need anti-retroviral (ARV) therapy but less than 20% of them can access treatment. As it stands, DWB provides around 80% of all freely available ARV treatment in the country (to more than 11,000 people), an untenable and unacceptable situation. Thus, DWB has had to make the difficult decision to severely restrict admissions to its HIV/AIDS program, while advocating strongly that the government of Myanmar and the international community urgently and rapidly scale-up ARV treatment. HIV is just one of a number of treatable epidemics that causes Myanmar to have some of the worst health statistics in Southeast Asia. Malaria remains the number one killer, with deaths in the country equaling more than half of those in Southeast Asia as a whole. Further, more than 80,000 new tuberculosis cases are detected each year, among the highest rates worldwide, and multidrug-resistant TB is on the rise.
ZIMBABWE: HEALTH CRISIS AND VIOLENCE
The first months of 2008 marked a period of further economic meltdown and political violence throughout Zimbabwe. While the country has been in crisis for years, the situation deteriorated to ever more alarming levels, with inflation of 231 million percent, shortages of essential goods, repression of opposition supporters, and additional restrictions on humanitarian organizations in the lead up to contested elections in June.
The crisis was especially troubling for the country’s estimated two million people living with HIV/AIDS. According to the United Nations, life expectancy in Zimbabwe has plummeted to just 34 years of age because of the HIV/AIDS pandemic. As a result of the crisis, many people undergoing treatment were forced to skip meals, unable to afford bus fares to clinics, or were simply too afraid to leave their homes. DWB has 40,000 people with HIV/AIDS under its care in Zimbabwe, half of them on anti-retroviral therapy. As patients missed appointments, some were feared to have fled the country. Unplanned treatment interruptions can have severe health consequences, including treatment failure due to the development of drug resistance.
Throughout the year, Zimbabweans continued to flee the country in alarming numbers. The flight of much-needed medical staff placed an even greater strain on the country’s deteriorating health-care system. About 3 million Zimbabweans have fled to neighboring South Africa; an unprecedented figure for a country not at war. Every day, thousands of people crossed the Limpopo River to reach the South African border town of Musina, risking beatings, rape, or robbery by bandits. DWB launched a project in the border town of Beitbridge to assist migrants on their way to South Africa and ran mobile clinics for new arrivals at sites along the Limpopo River and in Musina itself. Many who reached South Africa were forced to live underground to avoid arrest and deportation and in May, Zimbabweans, along with other foreign nationals, were targeted with violent xenophobic attacks, which displaced more than 100,000 people throughout South Africa. DWB provided emergency assistance to victims of the xenophobic violence.
The worst outbreak of cholera in years began in August and quickly spread as a result of the country’s collapsed infrastructure. The outbreak, which has been centered in Harare, was declared a national emergency in early December, by which time DWB had treated more than 11,000 patients. DWB’s medical teams set up more than a dozen cholera treatment centers and units, helped chlorinate water sources, disinfected homes, and sent teams throughout the countryside to treat outbreaks in rural areas. Significant new outbreaks were found in mid-December, particularly worrying as the rainy season had not yet started in many areas. Cholera spreads more easily in the rainy season, November to March, when contaminated sewage is more likely to be flushed into unprotected wells. DWB expects to be caring for cholera patients in Zimbabwe in 2009.
EASTERN CONGO: TRAPPED CIVILIANS
Since September 2007 renewed fighting in North Kivu has caused massive displacement in the region. A ceasefire agreement signed in January 2008 was not respected and, by the end of August, large-scale fighting had broken out again in the region between various armed groups and the Congolese armed forces (FARDC), despite the presence of the world’s largest UN peacekeeping force, MONUC.
Hundreds of thousands of people fled in all directions throughout the region, desperately in search of safety. The displaced, many of whom have been forced to flee multiple times, have little or no access to health care, food, water or basic shelter. They find shelter in camps or with host families, or hide in the forest where they are under threat of attack from all armed groups. Few aid agencies have established humanitarian programs with a continued presence outside the provincial capital, Goma.
Despite its UN mandate, MONUC has not been able to protect civilians from violence and forced displacement. In November, after rebel forces took control of Rutshuru, where DWB runs a surgical hospital, MONUC lead an armed “humanitarian relief” convoy into this town, a move that threatens to further blur the lines between military and humanitarian action in the region.
The displaced are also extremely vulnerable to easily treatable conditions and diseases such as measles, malnutrition, respiratory infections, diarrhea, and obstetrical complications. In addition, cholera cases are reported in different areas including places where this diarrheal disease is not usually a major health threat. Risk factors for contracting cholera include poor sanitation, lack of clean water, the constant movement of populations, and crowded conditions in displaced camps.
DWB is running projects throughout North and South Kivu provinces, providing emergency medical assistance, as well as primary and secondary health care, water and sanitation assistance, and distribution of essential items such as shelter materials and blankets. In particular, DWB is operating the hospital in Rutshuru and in November the team did not stop working when fighting broke out in the city and in the nearby town of Kiwanja.
DWB increased its emergency response in the region to cope with the deteriorating situation. As one of the few humanitarian organizations with teams based and working outside of Goma, DWB is exploring ways to increase its response to the crisis to meet the needs of the population. But due to insecurity and fighting, some areas remain inaccessible and people remain removed from any access to health care. Local families, who often take in those forced to flee, are bearing a huge burden to assist their displaced neighbors.
While media attention has focused on the fighting in North and South Kivu province, civilians living in Haut-Uele district have fallen prey to a series of cross-border raids by the rebel group, Lord’s Resistance Army, since October. Fighting in September forced some 50,000 people to flee their homes. And the Congolese population in other regions of the country endures a perpetual lack of access to health care and recurring epidemics, such as the cholera outbreak that sickened more than 4,000 people in Lubumbashi and Likasi in Katanga province, and a measles outbreak to which DWB responded with a vaccination campaign reaching more than 225,000 children between 6 months and 15 years old.
MALNUTRITION: 178 MILLION CHILDREN AFFECTED
Food riots around the world early in 2008 brought into sharp relief the impact of rising food prices on communities as far apart as Haiti, Bangladesh, and Ivory Coast. Less visible, though more deadly and pervasive, was the ongoing crisis in childhood malnutrition. While combating hunger depends on having access to food in sufficient quantity, conquering malnutrition also means assuring foods of adequate nutritional quality. For young, malnourished children, foods rich in nutrients, vitamins, and minerals are essential to survival and development.
The figures are shocking. The World Health Organization (WHO) estimates there are 178 million children suffering from undernutrition across the globe. All told, malnutrition contributes to 3.5 to 5 million deaths in children under five each year. According to UNICEF, the situation is actually getting worse in 16 high-burden countries. In the world’s “malnutrition hotspots,” the Horn of Africa, the Sahel and South Asia, many families simply cannot afford to provide nutritious food – particularly animal source foods such as milk, meat, and eggs – that young children need to grow and thrive. Instead, they struggle to survive – far from the media spotlight of high-profile humanitarian emergencies – on a diet of little more than cereal porridges of maize or rice, amounting to the equivalent of bread and water.
For the tens of millions of children who do receive assistance, international food aid and nutrition programs have had limited impact in preventing their downward spiral into life-threatening malnutrition. This failure is due to assistance programs built on foods that are nutritionally inappropriate to rehabilitate malnourished children. The main foods – fortified blended flours made from either corn or wheat plus soya – do not meet the minimum nutritional needs of the most vulnerable children between 6 and 24 months. DWB is advocating that governments and international agencies adjust the products in food aid to better meet the needs of the people it aims to help by providing child-appropriate foods of high nutritional value such as supplemental ready-to-use foods.
ETHIOPIA: DROUGHT AND CONFLICT
Continued violence and harsh climatic conditions have made living a constant struggle for people in the crisis-affected area of Ethiopia’s Somali region last year. Caught between rebel groups based in the region and government forces intent on quelling the rebellion, the largely nomadic population has become ever more isolated from basic services and humanitarian assistance.
Due to dangers and restrictions associated with importing goods to the region, the availability of food and other essential items in local markets has drastically decreased and price spikes made basic staples largely unaffordable. At the same time, severe restrictions on movements in certain zones have seriously increased the vulnerability of nomadic people who are unable to search for water and food for their livestock. People have seen their harvests, food stocks, grazing lands, and livestock destroyed by a combination of drought and as a result of the conflict. Some have been directly exposed to the violence.
In May, DWB discovered concerning rates of malnutrition in parts of the Somali region, corresponding to the unfolding nutritional crisis in southern Ethiopia. It also found diseases such as diarrhea, urinary tract and eye infections, indicative of inadequate water and sanitation. In Wardher, a town in eastern Somali region, DWB witnessed thousands of nomadic herders and bush-dwellers drawn to the town’s outskirts, in search of food, water, and health care.
In contrast to the difficulties in working in the Somali region, DWB was able to launch a massive response to the outbreak of malnutrition in Ethiopia’s Oromiya and Southern Nations and Nationalities People’s (SNNP) regions. From May to September, DWB treated more than 28,000 severely malnourished patients and 21,000 moderately malnourished patients across the different locations. Also in July, DWB made a targeted food distribution for 12,500 people at risk of malnutrition.
PAKISTAN: VICTIMS OF FIGHTING
The fighting between government forces and anti-government militants in the north west frontier province and the federally administered tribal areas of Pakistan has intensified throughout 2008. Air strikes by United States military in the area have also increased insecurity. In August, thousands of Pakistanis were displaced within the country or fled to neighboring Afghanistan for safety. At the same time, the Pakistani army also began expelling Afghan refugees, specifically in Bajaur Agency, for alleged connections to militant groups.
Throughout the course of the year, hundreds of people in the Bajaur Agency and Swat and Mohmand regions were killed or injured in suicide bombings, air attacks, and shootings, with thousands more repeatedly uprooted from their homes. DWB provided thousands of people with the basic materials they needed to survive: blankets, floor mats, shelter items, hygiene kits and food. DWB adapted its primary healthcare programs to respond to the sharp increase in victims of violence by providing medical supplies to treat war-wounded, assisting in referrals, and providing care for the treatment of watery diarrhea caused by the poor quality of water initially provided for the displaced.
As local health clinics began to close for fear of violence, DWB opened mobile clinics in partnership with local health providers, and established a clearly identifiable ambulance service to bring patients safely to hospitals.
During the many curfews imposed by the military, the DWB ambulance became the only vehicle allowed to travel around, transporting 700 patients over a 5-month period – primarily women in labor and victims of violence.
In October, a spike in violence sent hundreds of thousands en masse into neighboring regions over the course of just a few days. Fleeing air attacks and bombings, many found refuge in private homes, mosques, schools, and makeshift camps. As diarrhea broke out in camps, DWB assisted with water and sanitation while local health authorities provided basic medical care.
In Kurram Agency, providing assistance is increasingly difficult due to ongoing sectarian violence and insecurity due to outside armed groups operating in the area. DWB’s main activities have been the provision of mother and child health care, including emergency obstetric surgery and neonatal services. Insecurity means only the most critical patients will risk traveling to reach medical services.
In Baluchistan, DWB assists Afghan refugees through support to mother and child health care near Quetta. In the border town of Chaman where health actors are struggling to provide care for the residents of the city, it also assists the local population and patients coming from Afghanistan by providing reproductive health care, including emergency obstetrics, neonatal services, and nutritional support.
The eastern region of Baluchistan is rich in gas reserves, but poor in health care, with an internal conflict that has been simmering for more than 30 years. An emergency feeding program for children has been started by DWB in the eastern districts of Jafarabad and Nasirabad where, in three months, DWB treated more than 1,000 children for malnutrition. Besides the armed conflict, the mountainous region of northwestern Baluchistan was hit by a magnitude 6.4 earthquake on October 29. Most of the mud brick houses were destroyed with people forced to sleep out in the cold due to the damage and fear as aftershocks continued. The official death toll rose to approximately 300 people, with 35,000 injured and 40,000 left homeless. In addition to providing emergency medical support and relief supplies, DWB teams also provided mental health care for the affected communities.
SUDAN: TWO MAJOR EMERGENCIES
Sudan continued to be wracked by two major humanitarian emergencies in 2008 – the crisis in Darfur and the consequences of decades of civil war in the South. Darfur remained the site of the largest humanitarian aid operation in the world, with more than 80 organizations and 15,000 aid workers – including 2,000 DWB staff – providing assistance in a region where one-third of the population has been displaced by conflict. But despite international efforts, five years into the Darfur crisis, hundreds of thousands of people remain cut off from aid. Thousands more are at risk of losing assistance as a result of unstable frontlines, shifting alliances among armed factions, targeted attacks on aid workers, and increasing government restrictions on the provision of humanitarian assistance. Eleven aid workers were killed in Darfur in 2008 and 189 abducted, according to the UN.
Improving public health indicators mask the sad fact that, for most people in Darfur, their security situation deteriorated significantly in 2008. In February, a brutal raid in West Darfur’s northern corridor area was a cruel reminder of the early days of the conflict, as bombings, attack helicopters, and ground troops returned in force. Villages were burned and emptied, affecting about 50,000 people. Many people seek refuge in Darfur’s vast camps for internally displaced persons, but there is little safety in numbers. In Kalma camp, home to more than 90,000 people, DWB teams treated 65 patients suffering from gunshot wounds after fighting broke out within the camp. More than half of those admitted were women and children. Fighting between rebel and government troops throughout the year has left thousands displaced and cut off from assistance.
In southern Sudan, the UN estimates that 1.2 million people have returned home after 20 years of civil war. Those returning have found their home regions practically devoid of infrastructure, services, or health care. And even with a peace agreement, the regional tensions continue to be explosive. In February 2008, after an extremely violent attack near the town of Abyei, thousands of people fled to camps in northern Bahr-el-Ghazal State and an estimated 10,000 fled into the bush. In May, fighting virtually destroyed Abyei, displacing another 60,000 people. Right after the clashes, 140 war-wounded were treated by DWB teams. Approximately 300 malnourished children under 5 were admitted into a therapeutic feeding program. In December, new fighting broke out causing further displacement.
Throughout 2008, DWB’s 1,500 field staff in southern Sudan provided medical services in a region where, in addition to the ongoing violent attacks, malnutrition is prevalent; maternal mortality rates remain among the highest in the world; tuberculosis and kala-azar are ongoing problems; and large-scale outbreaks of meningitis, measles, cholera, and malaria are relentless. In the midst of all of this, humanitarian aid was conspicuously lacking, with some major donors having redirected their funds and the number of humanitarian agencies reducing due to a lack of resources. With census results not yet released, there is a risk that next July elections may be delayed and that violence will again flare up in the region.
IRAQ: FOUR MILLION DISPLACED
One of the greatest challenges facing independent humanitarian action today is that of reaching civilians caught in war and armed conflicts. Nowhere is this more frustratingly illustrated than in Iraq, where DWB has struggled to gain a meaningful foothold since the US-led invasion of 2003. Various military and political actors have sought to use and abuse humanitarian action for political purposes and in doing so have made humanitarian organizations a target for violent attacks. This has undermined the ability of DWB, and other neutral humanitarian organizations to address critical needs of the civilian population.
Four million people have been displaced by the war in Iraq, with 2 million of them trapped within the country itself, according to UN High Commissioner for Refugees and the Internal Displacement Monitoring Center of the Norwegian Refugee Council. There has been some improvement of security in Iraq in the past 18 months. Overall levels of violence have reduced and a changing political environment has emerged. Despite these changes, the situation in Iraq is uncertain and many people are still living under the threat of violence.
Bombings and sectarian violence continue, causing death and life-threatening injuries that require immediate and intensive medical attention. In addition to trauma, there are concerns regarding general health-care provision in Iraq. The Iraqi government has made recent efforts to develop health services, but there are still enormous gaps and thousands of Iraqis receive either no or insufficient medical care. This situation results from years of neglect of health services – particularly for primary health care – and the loss of medical staff who have fled Iraq out of fear of assassination or abduction.
HIV/TB: A DEADLY COMBINATION
Every year, tuberculosis (TB) kills about 1.7 million people and 9 million develop active disease. TB is on the rise in countries with high HIV rates, particularly in southern Africa, which has the highest rates of HIV. Tuberculosis is one of the leading causes of death for people living with HIV/AIDS, and in the past 15 years, new TB cases have tripled in countries with high HIV prevalence. People living with HIV/AIDS are up to 50 times more likely to develop active TB in a given year compared with HIV-negative individuals, and roughly a third of the 33 million people living with HIV/AIDS worldwide are infected with latent TB. Yet, in 2006, less than one percent of people living with HIV/AIDS were screened for TB.
While the treatment of HIV has received substantial global attention, people living with both HIV and TB have slipped mostly under the radar mainly because sensitive diagnostic tools are lacking and treatment for co-infected patients is complicated. While programs still focus on individual diseases, patients may have both and other diseases.
Treatment for TB is outdated and complicated in itself and not adapted to the specific problems of co-infected patients. Health-care providers have to use at least four TB drugs initially. Sometimes these drugs have side effects, including nausea, vomiting, neuropathy, hepatitis, and others. If the drugs do not cause side effects, then clinicians must ensure that they are not negatively impacting the effects of the HIV medications the patient is also taking. No new TB drugs have been developed for global or large-scale use in decades and the increase in drug resistant cases of TB adds another dimension of complexity.
Perhaps most importantly, global donors, as well as national governments, must invest in new diagnostics and treatments to really begin to face this growing health threat. DWB is calling for a massive scale up in research and development of TB medicines and diagnostic tools, and vaccines. Around $2 billion needs to be invested annually in the development of new tools for TB, but only an estimated $429 million was invested in 2006, according to the Treatment Action Group.
* Excerpts from the 2008 report of Médecins Sans Frontières, created in 1971 by a small group of French doctors. This secular humanitarian-aid non-governmental organization, best known for its projects in war-torn regions and developing countries facing endemic diseases is now governed by an international board of directors located in Geneva, Switzerland, and organized into 20 sections. Known in United States and Canada by its English name, Doctors Without Borders was awarded, in 1999, the Nobel Peace Award. Annually, about 3,000 doctors, nurses, midwives and logisticians are recruited to run projects, but 1,000 permanently employed staff work to recruit volunteers and handle finances and media relations. Private donors provide about 80% of the organization’s funding, while governmental and corporate donations provide the rest, giving the organization an annual budget of approximately $400 million. (www.doctorswithoutborders.org)